Chief Technology Solutions
Thank you for your interest in Chief Technology Solutions. As of April 2021 we are no longer accepting new clients.
Featured Research
Free Resources
Download now: Get the Digital Workplace Buyers Guide
Other Research
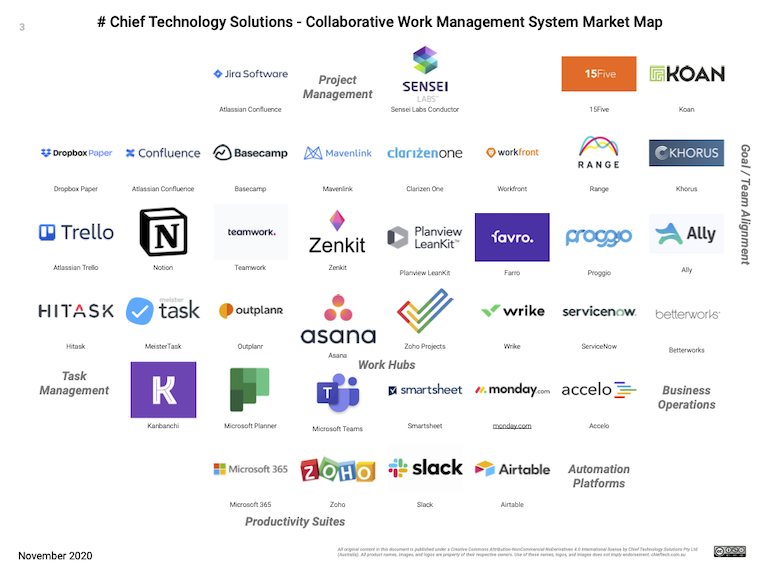
Focus area: Collaborative Work Management
On CMSWire & Reworked

More Featured Content and Resources
Featured Work: Creating the Future of Work Story
Recommended Posts:
- Every Abstraction Layer Erases an Apprenticeship: A Socio-Technical Look at Expertise
- Creating the Future of Work Story
- Solving the Collaborative Work Management Puzzle
- Notes about digital placemaking for the workplace
Explore more blogposts.